Clinical Support
In a proof-of-concept study involving 100 patients, 98% of all patients improved, with 42% of patients improving after just a single treatment with L-PACT!
We are developing a new evidence-based approach for CLBP management
Back pain is the leading cause of disability. Yet, today’s treatments for CLBP management are high-risk, costly and not efficient enough.
We believe there is a better way that focusses on treating the cause, not just the symptoms, to improve long-term quality of life.
Addressing the limitations of today’s most common treatments for CLBP
Today, opioids are the most prescribed drug class in the US for low back pain, with more than half of regular opioid users reporting back pain. With a high risk of addiction and overdose related mortality (46 people die per day), the opioid crisis is driving healthcare providers to find new treatment approaches for CLBP.
With traditional physical therapy challenged by low adherence and high patient costs from lengthy sessions, there is a clear need for alternative non-invasive therapies for CLBP.
Prescribing NSAIDs,
steroids, and opioids
- Adverse effects
- Risk of addiction
Low back pain,
imaging and surgeries
- Costly
- Low success rate
- Risk of complications
Lengthy
physical therapy
- Low adherence
- Lengthy, costly
- Challenging management
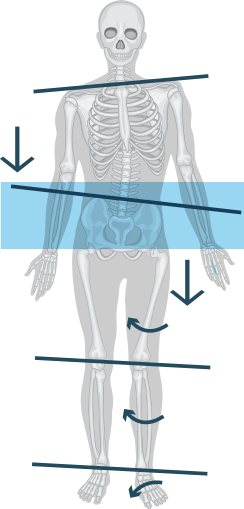
What happens in CLBP?
The human skeleton is a complex functional machine that constantly interacts with the force of gravity to maintain balance, allow coordinated movement and absorb impact. These vertical forces are absorbed by the spine which distributes them through the pelvis to the lower extremities.
The Lumbo-Pelvic junction serves as a Load Distribution Axis (LDA) which translates spinal axial loads evenly through the legs, to the ground to maintain a neuro-mechanical efficient centre of gravity.
Over time, physical loads, and motion patterns, asymmetrical pelvic postural motion may occur, due to minor physical traumas, bad postural habits, daily living activity efforts etc…, these can lead to Lumbo-Pelvic postural imbalances
Chronic imbalances, caused by even minor asymmetrical LDA, leads over time to Pelvic Dynamic Postural Imbalance and dysfunction which in turn may develop to CLBP.
Our approach

The L-PACT technology targets the functional root cause by restoring the correct loading of lumbar spinal structures to reduce pain and musculoskeletal degeneration for long-term prevention. The device neuro-mechanically trains the body to achieve correct Postural Dynamic Balance during short sessions of walking.
As a fully automated, wearable device enabling easy follow-up and short treatment, the L-PACT offers a highly accessible first-line treatment of choice for self- or guided-treatment, prevention and a scalable solution for CLBP.
Alongside saving clinician’s time and increasing efficiency so more patients can be treated faster, the L-PACT also improves evidence-based results and enables uniformity of assessment.

Supporting scientific literature
The L-PACT’s novel technology was developed based on years of research performed in the field. Below is key research published in leading peer-reviewed journals that supports this unique methodology to reduce CLBP and long-term deterioration by correcting asymmetries in the lumbo-pelvic movement and posture.
- Yu, Q., Huang, H., Zhang, Z., Hu, X., Li, W., Li, L., Chen, M., Liang, Z., Lo, W. L. A., & Wang, C. (2020). The association between pelvic asymmetry and non-specific chronic low back pain as assessed by the global postural system. BMC Musculoskeletal Disorders, 21(1), 596. doi: 10.1186/s12891-020-03596-5.
- Don Tigny, R. L. (2020). Evidence of errors that have stymied low back pain. International Journal of Complementary & Alternative Medicine, 13(6), 252-257. doi: 10.15406/ijcam.2020.13.00524.
- Tatsumi, M., Mkoba, E. M., Suzuki, Y., Kajiwara, Y., Zeidan, H., Harada, K., Bitoh, T., Nishida, Y., Nakai, K., Shimoura, K., & Aoyama, T. (2019). Risk factors of low back pain and the relationship with sagittal vertebral alignment in Tanzania. BMC Musculoskeletal Disorders, 20(1), 584. doi: 10.1186/s12891-019-2968-3.
- Król, A., Polak, M., Szczygieł, E., Wójcik, P., & Gleb, K. (2017). Relationship between mechanical factors and pelvic tilt in adults with and without low back pain. Journal of Back and Musculoskeletal Rehabilitation, 30(4), 699-705. doi: 10.3233/BMR-140177.
- Klima, S., Grunert, R., Ondruschka, B., Scholze, M., Seidel, T., Werner, M., & Hammer, N. (2018). Pelvic orthosis effects on posterior pelvis kinematics: An in-vitro biomechanical study. Scientific Reports, 8(1), 15980. doi: 10.1038/s41598-018-34360-6.
- Laird, R. A., Gilbert, J., Kent, P., & Keating, J. L. (2014). Comparing lumbo-pelvic kinematics in people with and without back pain: a systematic review and meta-analysis. BMC Musculoskeletal Disorders, 15(1), 229. doi: 10.1186/1471-2474-15-229.
- Buganè, F., Benedetti, M. G., D’Angeli, V., & Leardini, A. (2014). Estimation of pelvis kinematics in level walking based on a single inertial sensor positioned close to the sacrum: validation on healthy subjects with stereophotogrammetric system. BioMedical Engineering OnLine, 13(1), 146. doi: 10.1186/1475-925X-13-146.
- Kim, D.-H., Park, J.-K., & Jeong, M.-K. (2013). Influences of posterior-located center of gravity on lumbar extension strength, balance, and lumbar lordosis in chronic low back pain. Journal of Back and Musculoskeletal Rehabilitation, 26(4), 345-350. doi: 10.3233/BMR-130442.
- Al-Eisa E., Egan D., Deluzio K & Wassersug R. (2006). Effects of pelvic asymmetry and low back pain on trunk kinematics during sitting: a comparison with standing. Spine (Phila Pa 1976) Mar 1;31(5):E135-43. doi: 10.1097/01.brs.0000201325.89493.5f.
- Fleiss H., Fleiss O., Holzer P., Ritter G., & Stokes P. Gait pattern and spinal movement in walking: A therapeutic approach to low back pain.